
細野菜穂子ほか. 臨床血液. 2024; 65(5), 353-61.より作図.
ご監修:宮本 敏浩先生(金沢大学医薬保健研究域医学系 血液内科学 教授)
近年、次世代シーケンサー技術の進歩などにより、AMLの様々な遺伝子変異に起因する病態解明、治療標的分子の同定が進んでいます。今回は、国内外の最新の診療ガイドラインから、AMLにおけるTargeted therapyの考え方について解説します。



AMLに対する主な分子標的治療薬

AMLでは、FLT3阻害薬をはじめとする様々な分子標的治療薬が開発、上市されています(2025年2月時点)。上市されているものとして、国内ではFLT3阻害薬とBCL-2阻害薬、抗CD33抗体、米国ではこれらのほかIDH1/2阻害薬、メニン阻害薬があり、開発中のものはMDM2阻害薬、抗TIM-3抗体などがあります。

初発AMLに対するガイドライン
初発AMLに対する治療パラダイム(米国)

様々な分子標的治療薬の開発が進められるなか、現在のTargeted therapyの考え方を解説します。まず、初発のAMLに対する診断、治療についてです。現在の米国での治療パラダイムでは、強力な化学療法が可能な患者さんには、従来の7+3が行われますが、最近では治療標的となりうるバイオマーカーの発現状況により治療を上乗せするアプローチが行われるようになっています。例えば、FLT3遺伝子変異陽性例に対する初回寛解導入療法は、7+3にFLT3阻害薬を上乗せすることとされています。
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Acute Myeloid Leukemia Version 2.2025
Intensive Induction Eligible(Age ≥18 years)

NCCNガイドラインにおいても、FLT3遺伝子変異陽性例に対する初回寛解導入療法では、7+3にFLT3阻害薬を上乗せすることとされており、この治療はカテゴリー1で推奨されています。
診断時AMLに対するELN recommendations

Döhner H, et al.: Blood. 2022; 140(12), 1345-1377.より作図. 本論文の研究資金はAstellas Pharmaから提供を受けたものである。
ELN recommendationsにおいても、診断時に遺伝子検査を行うこととされており、初発AMLに対して治療標的となるバイオマーカーの発現の有無を確認した上でのTargeted therapyが行われています。
再発・難治AMLに対するガイドライン
再発・難治AMLに対するELN recommendations、NCCN Guidelines

1)Döhner H, et al.: Blood. 2022; 140(12), 1345-1377.より作図. 本論文の研究資金はAstellas Pharmaから提供を受けたものである。
2)NCCN Clinical Practice Guidelines in Oncology. Acute Myeloid Leukemia. Version 1.2025.より作図.
3)NCCN Clinical Practice Guidelines in Oncology. Acute Myeloid Leukemia. Version 3.2024.より作図.
再発・難治AMLに対するTargeted therapyの考え方を解説します。
ELN recommendationsでは、再発・難治AMLに対して、clonal evolutionや、診断時に検出されなかったクローンが出現している可能性を考慮して、改めて分子遺伝学的検査で評価することの重要性が述べられています1)。NCCNガイドラインでは、再発や進行を認めたら、その都度繰り返し遺伝子検査を行うべきであると述べられています。再発、進行時の検査については、2024年のversion 3では網羅的な遺伝子検査で変異の有無を検討するように記載されていましたが、2025年のversion 1ではactionable mutationを検出する遺伝子検査へと記載が変更されました2、3)。
NCCN Guidelines for Acute Myeloid Leukemia Version 2.2025
Therapy FOR Relapsed/Refractory DISEASEi,yy (Age ≥18 years)
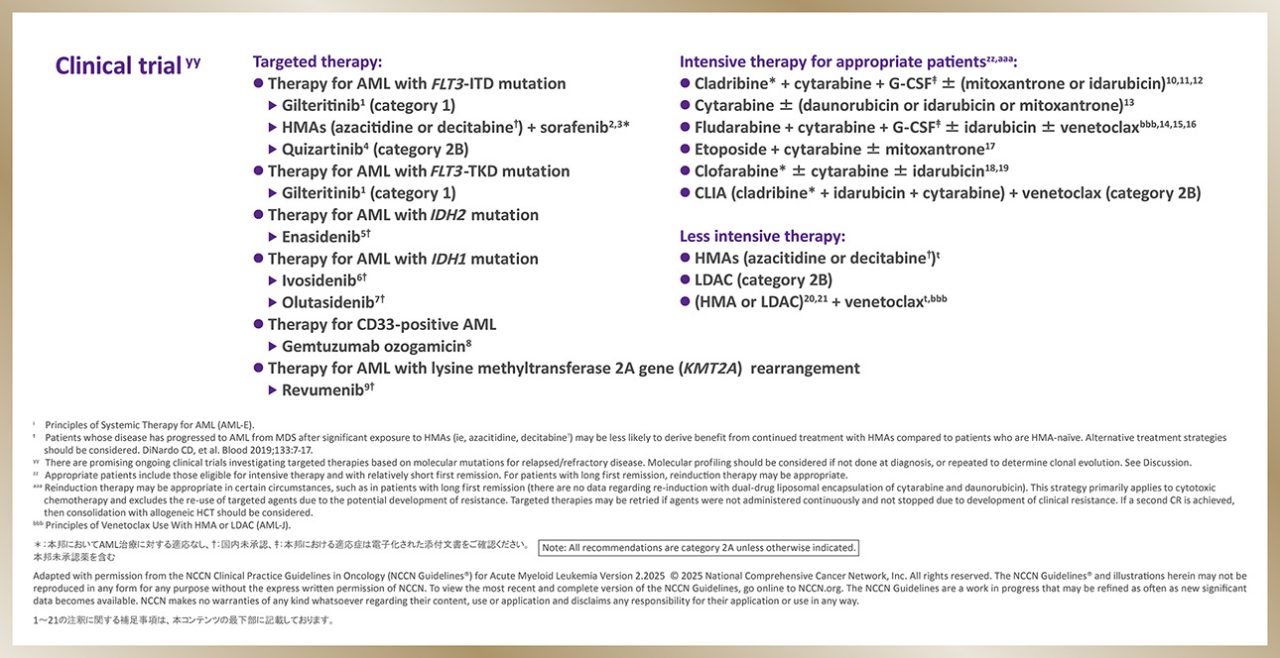
NCCNガイドラインでは、再発・難治AMLの治療においてもTargeted therapyが推奨されています。
初発のFLT3遺伝子変異陽性AMLに7+3とFLT3阻害薬の併用療法が推奨されていることを先述しましたが、再発・難治例においても、FLT3阻害薬がカテゴリー1または2で推奨されており、ゾスパタはカテゴリー1で推奨されています。

本邦で承認されたAMLに対する分子標的治療薬

日本の状況を踏まえると、海外でのTargeted therapyの考え方は本邦でも適用しうると考えられます。
化学療法だけではなく、FLT3阻害薬やBCL-2阻害薬、抗CD33抗体が登場し、治療選択肢が広がった状況は海外と同様です。初発AMLに対して、本邦でもBCL-2阻害薬、FLT3阻害薬による治療が可能となっています。
造血器腫瘍診療ガイドライン(日本血液学会:2024年版)
若年者AMLの治療アルゴリズム

一般社団法人 日本血液学会. 造血器腫瘍診療ガイドライン第3.1版(2024年版). http://www.jshem.or.jp/gui-hemali/table.html (2024年12月閲覧)
現在、国内のガイドラインでは、再発・難治例においてはFLT3遺伝子変異の情報を取得し、陽性例に対しては、CQ9でFLT3阻害薬を用いることが勧められており、2種類のFLT3阻害薬、ゾスパタとキザルチニブによる治療が可能であるとされています。
まとめ


1)Döhner H, et al.: Blood. 2022; 140(12), 1345-1377. 本論文の研究資金はAstellas Pharmaから提供を受けたものである。
2)NCCN Clinical Practice Guidelines in Oncology. Acute Myeloid Leukemia. Version 1.2025.
3)NCCN Clinical Practice Guidelines in Oncology. Acute Myeloid Leukemia. Version 3.2024.
FOOTNOTES FOR INTENSIVE INDUCTION ELIGIBLE
a Patients with elevated blast counts are at risk for tumor lysis and organ dysfunction secondary to leukostasis. Measures to rapidly reduce the WBC count include leukapheresis, hydroxyurea, and/or a single dose of cytarabine. Prompt institution of definitive therapy is essential.
b Poor performance/functional status and a comorbid medical condition, in addition to age, are factors that influence ability to tolerate standard induction therapy. Web- based tools available to evaluate the probability of CR and early death after standard induction therapy in patients aged ≥60 years with AML can be found at: Walter RB, et al. J Clin Oncol 2011;29:4417-4423; Borlenghi E, et al. J Geriatr Oncol 2021;12:550-556. Consider the use of geriatric assessment for patients with AML ≥60 years of age. Ritchie EK, et al. Blood Adv 2022;6:3812-3820; Min GJ, et al. Blood 2022;139:1646-1658; Saad M, et al. Blood 2020;136:2715-2719; Klepin HD, et al. Blood 2013;121:4287-4294. See NCCN Guidelines for Older Adult Oncology.
c Consider screening with FISH to identify translocations/abnormalities associated with CBF-AML.
d In-frame bZIP mutations in CEBPA are more predictive of favorable outcomes than double mutations. Taube F, et al. Blood 2022;139:87-103; Wakita S, et al. Blood Adv 2022;6:238-247; Tarlock K, et al. Blood 2021;138:1137-1147.
e Principles of Supportive Care for AML (AML-F).
f Monitoring During Therapy (AML-G).
g Consider referral to palliative care for consultation at the start of induction. El-Jawahri A, et al. JAMA Oncol 2021;7:238-245. See NCCN Guidelines for Palliative Care.
h General Considerations and Supportive Care for Patients with AML Who Prefer Not to Receive Blood Transfusions (AML-D).
i Principles of Systemic Therapy for AML (AML-E).
j For patients who exceed anthracycline dose or have cardiac issues but are still able to receive intensive therapy, alternative non-anthracycline–containing regimens may be considered (eg, FLAG, clofarabine*-based regimens [category 3]). See Discussion.
k For CBF-AML with FLT3-TKD mutation, the Panel prefers gemtuzumab ozogamicin over an FLT3 inhibitor.
l Patients who receive transplant shortly following gemtuzumab ozogamicin administration may be at risk for developing sinusoidal obstruction syndrome (SOS). Wadleigh M, et al. Blood 2003;102:1578-1582. If transplant is planned, note that prior studies have used a 60- to 90-day interval between the last administration of gemtuzumab ozogamicin and HCT.
m Threshold for CD33 is not well-defined and may be ≥1% by flow cytometry.
n In times of fludarabine shortage, cladribine* can be substituted for fludarabine.
o Gemtuzumab ozogamicin may be beneficial in NPM1-mutated AML (Kapp-Schwoerer S, et al. Blood 2020;136:3041-3050). The role of gemtuzumab ozogamicin in CEBPA-mutated AML is not established.
p The RATIFY trial studied patients aged 18–60 y with FLT3-mutated AML. An extrapolation of the data suggests that patients aged 61–70 years with FLT3-mutated AML who are fit to receive 7 + 3 should be offered midostaurin since it seems to provide a survival benefit without undue toxicity. Schlenk RF, et al. Blood 2019;133:840-851.
*:本邦においてAML治療に対する適応なし
REFERENCES FOR THERAPY FOR RELAPSED/REFRACTORY DISEASE
1 Perl AE, Larson RA, Podoltsev NA, et al. Follow-up of patients with R/R FLT3-mutation-positive AML treated with gilteritinib in the phase 3 ADMIRAL trial. Blood 2022;139:3366-3375.
2 Ravandi F, Alattar ML, Grunwald MR, et al. Phase 2 study of azacytidine plus sorafenib in patients with acute myeloid leukemia and FLT3 internal tandem duplication mutation. Blood 2013:121:4655-4662.
3 Muppidi MR, Portwood S, Griffiths EA, et al. Decitabine and sorafenib therapy in FLT3 ITD-mutant acute myeloid leukemia. Clin Lymphoma Myeloma Leuk 2015;15 Suppl:S73-9.
4 Cortes JE, Khaled S, Martinelli G, et al. Quizartinib versus salvage chemotherapy in relapsed or refractory FLT3-ITD acute myeloid leukaemia (QuANTUM-R): a multicentre, randomised, controlled, open-label, phase 3 trial. Lancet Oncol 2019;20:984-997.
5 Stein EM, DiNardo CD, Pollyea DA, et al. Enasidenib in mutant IDH2 relapsed or refractory acute myeloid leukemia. Blood 2017;130:722-731.
6 DiNardo CD, Stein EM, de Botton S, et al. Durable remissions with ivosidenib in IDH1-mutated relapsed or refractory AML. N Eng J Med 2018;378:2386-2398.
7 Cortes J, Fenaux P, Yee K, et al. Olutasidenib (FT-2102) induces durable complete remissions in patients with relapsed/refractory mIDH1 acute myeloid leukemia. Results from a planned interim analysis of a phase 2 pivotal clinical trial[abstract] Blood 2022;140: Abstract 2757.
8 Taksin AL, Legrand O, Raffoux E, et al. High efficacy and safety profile of fractionated doses of Mylotarg as induction therapy in patients with relapsed acute myeloblastic leukemia: a prospective study of the alfa group. Leukemia 2007;21:66-71.
9 Issa GC, Aldoss I, Thirman MJ, et al. Menin inhibition with revumenib for KMT2A rearranged relapsed or refractory acute leukemia (AUGMENT-101). J Clin Oncol 2024:JCO2400826.
10 Robak T, Wrzesień-Kuś A, Lech-Marańda E, et al. Combination regimen of cladribine (2-chlorodeoxyadenosine), cytarabine and G-CSF (CLAG) as induction therapy for patients with relapsed or refractory acute myeloid leukemia. Leuk Lymphoma 2000;39:121-129.
11 Fridle C, Medinger M, Wilk MC, et al. Cladribine, cytarabine and idarubicin(CLA-Ida) salvage chemotherapy in relapsed acute myeloid leukemia (AML). Leuk Lymphoma 2017:1068-1075.
12 Wrzesien-Kus A, Robak T, Wierzbowska A, et al. A multicenter, open, noncomparative, phase II study of the combination of cladribine(2-chlorodeoxyadenosine), cytarabine, granulocyte colony-stimulating factor and mitoxantrone as induction therapy in refractory acute myeloid leukemia: a report of the Polish Adult Leukemia Group. Ann Hematol 2005;84:557-564.
13 Karanes C, Kopecky KJ, Head DR, et al. A phase III comparison of high dose ARA-C (HIDAC) versus HIDAC plus mitoxantrone in the treatment of first relapsed or refractory acute myeloid leukemia Southwest Oncology Group Study. Leuk Res 1999;23:787-794.
14 Montillo M, Mirto S, Petti MC, et al. Fludarabine, cytarabine, and G-CSF (FLAG) for the treatment of poor risk acute myeloid leukemia. Am J Hematol 1998;58:105-109.
15 Parker JE, Pagliuca A, Mijovic A, et al. Fludarabine, cytarabine, G-CSF and idarubicin (FLAG-IDA) for the treatment of poor-risk myelodysplastic syndromes and acute myeloid leukaemia. Br J Haematol 1997;99:939-944.
16 DiNardo CD, Lachowiez CA, Takahashi K, et al. Venetoclax combined with FLAG-IDA induction and consolidation in newly diagnosed and relapsed or refractory acute myeloid leukemia. J Clin Oncol 2021;39:2768-2778.
17 Nair G, Karmali G, Gregory SA, et al. Etoposide and cytarabine as an effective and safe cytoreductive regimen for relapsed or refractory acute myeloid leukemia[abstract]. J Clin Oncol 2011;29(Suppl):Abstract 6539.
18 Faderl S, Wetzler M, Rizzieri D, et al. Clorarabine plus cytarabine compared with cytarabine alone in older patients with relapsed or refractory acute myelogenous leukemia: results from the CLASSIC I Trial. J Clin Oncol 2012;30:2492-2499.
19 Faderl S, Ferrajoli A, Wierda W, et al. Clofarabine combinations as acute myeloid leukemia salvage therapy. Cancer 2008;113:2090-2096.
20 Aldoss I, Yang D, Aribi A, et al. Efficacy of the combination of venetoclax and hypomethylating agents in relapsed/refractory acute myeloid leukemia. Haematologica 2018;103:e404-e407.
21 DiNardo CD, Rausch CR, Benton C, et al. Clinical experience with the BCL2-inhibitor venetoclax in combination therapy for relapsed and refractory acute myeloid leukemia and related myeloid malignancies. Am J Hematol 2018;93:401-407.
関連する製品情報
アステラス製薬株式会社の医療関係者向け情報サイトにアクセスいただき、ありがとうございます。
アステラスメディカルネット会員の方
medパス会員の方
medパスのパスワード再発行をご希望の場合も上記よりアクセスください。
会員登録されていない方
医療従事者の方は、会員限定コンテンツを除いたアステラスメディカルネットサイトの一部をご覧いただけます。
会員登録すると、製品に関する詳細な情報や領域ごとの最新情報など、会員限定のコンテンツが閲覧できます。
会員向けコンテンツをご利用の方
会員になると以下のコンテンツ、サイト機能をご利用いただけます。

